According to a new
study published online in Radiology, a large percentage of patients who receive
radiologist recommendations for Chest CT have clinically relevant
findings. The findings thus demonstrate
that radiologist recommendations for additional imaging (RAIs) after chest
x-rays represent valuable contributions to patient care.
RAIs have shown a tremendous growth rate of 200 percent since 1995. This massive growth has attracted scrutiny since healthcare is moving from volume-driven to value-based payment models. Emphasis is being made to ensure that the radiology community validates the clinical impact of its work.
According to study author Tarik K. Alkasab, MD, PhD, from Massachusetts General Hospital and Harvard Medical School in Boston, “There has been a great deal of research on how radiologists recommend an imaging exam, but little on what comes out of the exams that they recommend. Prior studies were very broad, so in our study we tried to focus on a specific clinical scenario.
Chest x-rays are the
most commonly performed outpatient diagnostic imaging studies in the US. Nearly
half of all RAIs arising from thoracic diagnostic exams are prompted by chest x-rays.
During the study, the research team
evaluated more than 29,000 reports of outpatient chest x-rays that had been
performed at a large academic centre over a period of one year.
They found that radiologists
interpreting outpatient chest x-rays made recommendations for CT in 4.5 percent
of cases. In 41.4 percent of the chest CTs, a corresponding abnormality was detected
that required treatment or further diagnostic workup. One in every 13 yielded a
corresponding abnormality representing a newly-diagnosed, biopsy-proven
malignancy.
According to study
co-author H. Benjamin Harvey, M.D., J.D., from Massachusetts General Hospital
and Harvard Medical School, these findings clearly show that the risk of
radiation-induced cancer associated with a chest CT is of much less magnitude
than the potential benefits of it. If the ordering physician sees a
recommendation for chest CT, he should ensure that the patient gets the
recommended imaging. The study showed that approximately one-third of patients in
the study group who were recommended for follow-up chest CT did not receive the
exam. The researchers point out that such oversight could result in missed or
delayed diagnoses.
“More research is needed to understand the
possible reasons for the less-than-optimal adherence to RAIs after chest
X-ray,” Dr. Harvey said. “One thing we’re looking at is how the recommendation
language affects recommendation adherence.”
The study team is
hopeful that the findings will help improve the awareness of the importance of follow
up chest CT. It is important for radiologists to be confident that their
recommendations are valuable and are necessary for the long-term health of their
patients.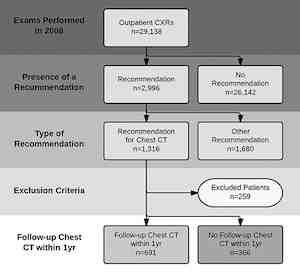
Figure 1. Schematic representation of the patient selection process. CXR = chest radiographic examination.
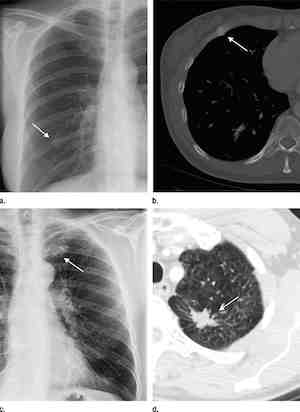
Figure 2. Examples
of lesions seen on chest radiographic images that prompted a
recommendation for chest CT examination and the corresponding
abnormality on chest CT. (a, b) In the first example, a nodular opacity
(arrow on a) is seen projecting over the right posterior ninth rib in
the chest radiographic image of a 50-year-old woman who presented with
cough; the recommended chest CT examination demonstrated this to be
callus from a remote rib fracture (arrow on b). (c, d) In the second
example, a nodular opacity (arrow in c) is seen projecting over the left
anterior first rib on the chest radiographic image of a 53-year-old man
who is a former smoker and presented with cough; the recommended chest
CT examination demonstrated this to be a suspicious nodule in the
apicoposterior segment of the left upper lobe (arrow in d). On
resection, this was found to be well-differentiated adenocarcinoma of
the lung.
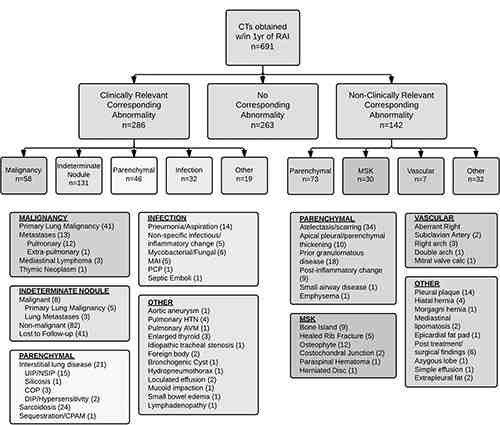
Figure 3. Schematic representation of the results of follow-up chest CT examinations performed within 1 year of the index outpatient chest radiographic examinations that contained the RAI. AVM = arteriovenous malformation, calc = calcification, COP = cryptogenic organizing pneumonia, CPAM = congenital pulmonary airways malformation, DIP = desquamative interstitial pneumonia, HTN = hypertension, MAI = Mycobacterium avium intracellulare, MSK = musculoskeletal, NSIP = nonspecific interstitial pneumonia, PCP = Pneumocystis pneumonia, UIP = usual interstitial pneumonia.
Source: Radiological Society of North America
Image Credit: Radiological Society of North America